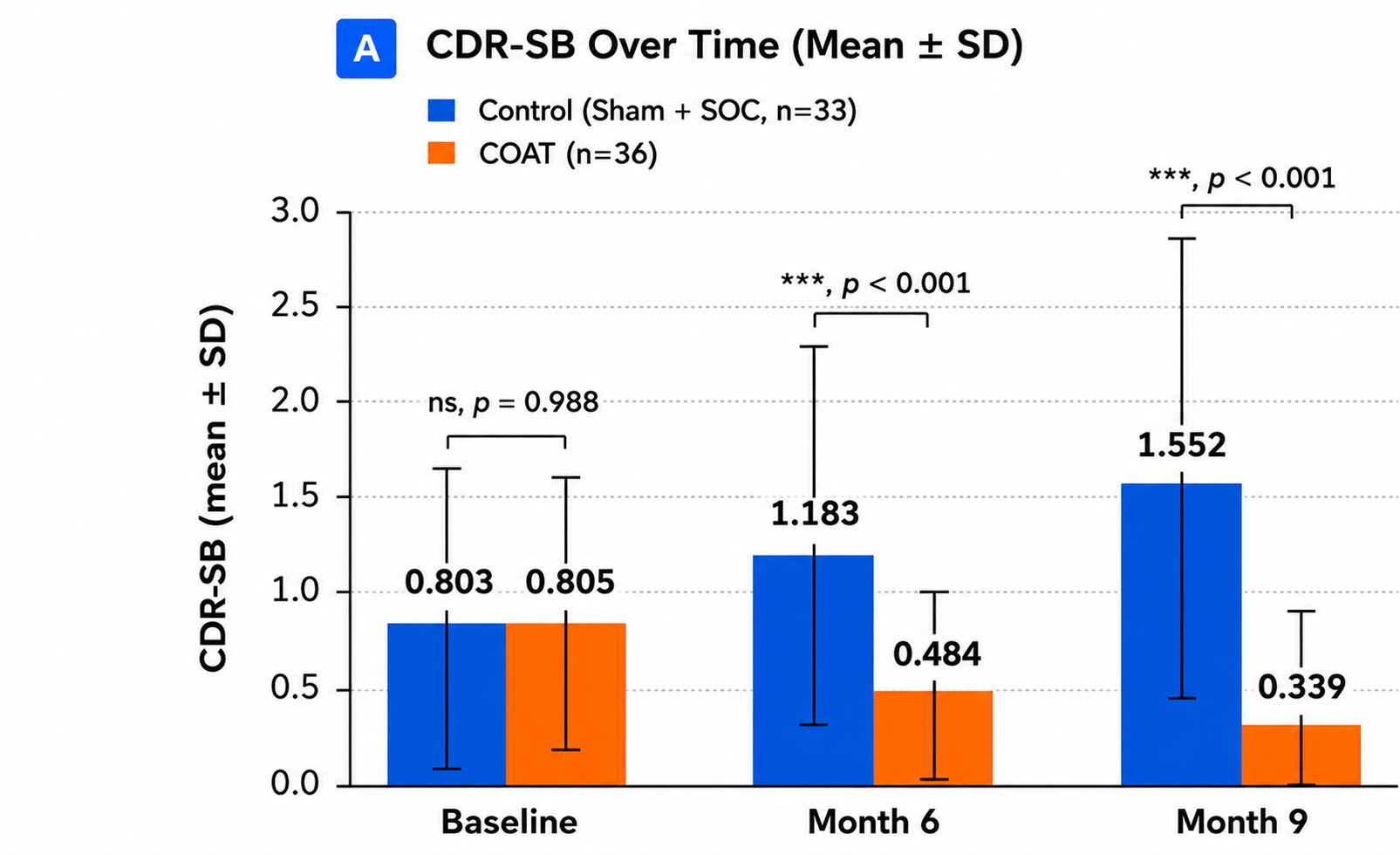
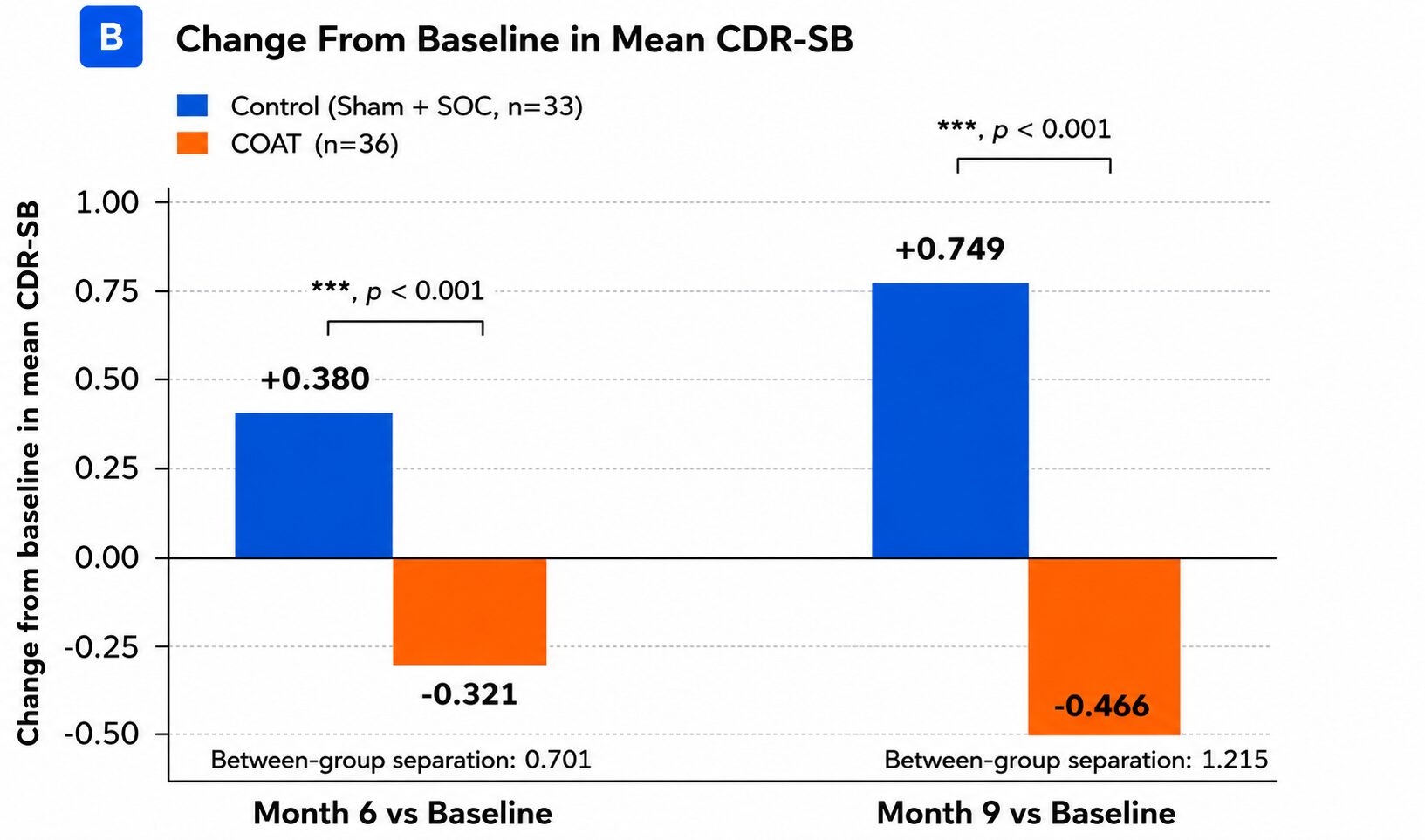
In plain terms: by month 9, people using COAT were, on average, holding steady or improving slightly on this scale — while the control group’s scores nearly doubled, reflecting the clinical decline typically seen in untreated early Alzheimer’s. (This CDR-SB analysis is pending peer-reviewed publication.)